Source: CMSA Today

In an article I wrote for Nursing Clinics of America, I highlighted the critical role of effective care transitions for chronic wound patients, emphasizing the need for robust communication between acute, skilled nursing and community-based care settings. By focusing on nurse and nurse practitioner (NP)-led community-based initiatives and strategies that reduce hospital readmissions, I am advocating for comprehensive discharge planning and sustained follow-up care. These efforts help mitigate complications and improve patient outcomes, particularly for older adults reliant on community and home-based care. I underscored the importance of interdisciplinary and inter-facility collaborations in managing chronic wounds more efficiently.
TRANSITION OF CARE FOR CHRONIC WOUNDS
Effective transitions of care for chronic wound patients are vital to ensure seamless continuity between hospital and community-based settings. By aligning acute care providers with home-based teams, clinicians can create individualized care plans emphasizing consistent wound management, patient education and timely follow-ups. Standardized communication protocols and digital tools, like shared electronic health records, enhance collaboration across disciplines, ensuring patients receive comprehensive, uninterrupted care tailored to their needs.
Community-based settings for chronic wound care, as highlighted in “Post-Acute Transitional Services: Safety in Home-Based Care Programs,” are pivotal in ensuring patient safety and improving outcomes. These settings include services provided by home health agencies (HHAs) and home-based primary care (HBPC) programs tailored to meet the needs of patients transitioning from hospital or skilled nursing facilities to home environments.
HHAs provide on-the-ground wound care, patient education and caregiver training to promote healing and prevent complications. However, they face challenges such as varying quality of care, inconsistent adherence to evidence-based practices and challenges of rehospitalization due to factors like insufficient caregiver skills or simply fewer community-based settings that will accept chronic and complex wounds such as stage 3 or 4 pressure injuries. In California, congregate living health facilities (CLHFs) that can manage these complex cases are few and far between.
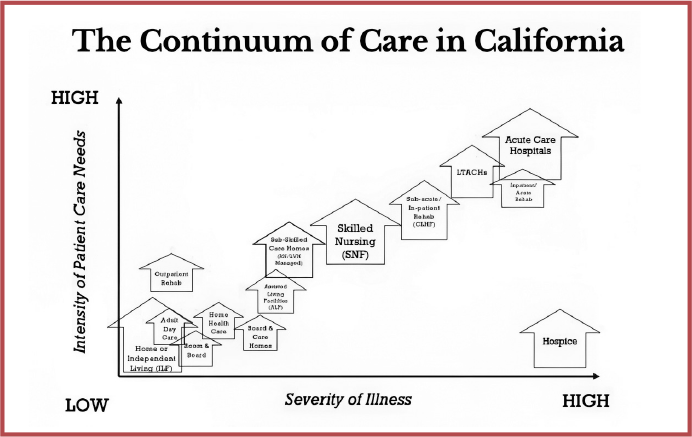
CARE SETTINGS: A CALIFORNIA EXAMPLE
There are approximately only about 200 CLHFs in all of California. Based on available data, estimating the number of patients with complex wounds in California involves extrapolation. In the UK, research estimates the prevalence of complex wounds to be around 16.4 per 10,000 people in community settings. Applying a similar prevalence to California’s population of approximately 39 million would suggest around 63,960 patients with complex wounds. However, regional differences in healthcare systems, demographics and underlying conditions may influence the accuracy of this figure. This estimate aligns with global trends where aging populations and rising chronic conditions such as diabetes contribute to a growing number of complex wound cases. Factors like improved healthcare access and reporting mechanisms could further refine these estimates, which is roughly a ratio of 1 facility for every 300 patients needing this type of facility care.
Source: Ordona, R. B. (2024). Transition of care challenges and opportunities for chronic wounds. Nursing Clinics of North America. https://doi.org/10.1016/j.cnur.2024.07.014
HBPC programs, initially designed for veterans, offer a multidisciplinary approach that includes in-home visits by healthcare professionals for patients with complex medical needs. These programs emphasize convenience for homebound patients and leverage advanced technology, like portable diagnostic tools, to deliver high-quality care directly in patients’ homes. These efforts address chronic wound management, reduce healthcare costs and improve access to care for medically complex individuals.
Efforts like the Home Health Value-Based Purchasing (HHVBP) initiative incentivize quality improvements in home-based care by shifting focus from volume-based to value-based models. This approach encourages better communication, comprehensive patient assessments and integration of technology, which are critical for chronic wound patients transitioning to community-based care settings.
In California, there are myriad choices as far as the continuum of care, post-acute or post-SNF care. There are complexities in ensuring patient safety and high-quality care in group home environments, particularly during unplanned incidents. Group homes often cater to individuals with significant medical or behavioral needs, necessitating a well-trained and appropriately staffed workforce. However, staffing shortages and gaps in preparedness for emergencies can compromise the quality of care and increase risks for residents.
In community-based settings, there is a need for proactive planning to address unplanned incidents, such as medical emergencies, behavioral crises or natural disasters, in group home settings. Inadequate staffing levels and training can lead to delayed responses and adverse outcomes. The development of contingency plans, routine emergency drills and staff education programs to improve readiness and ensure the safety of residents cannot be overemphasized. The integration of technologies, such as alarm systems and communication tools, can enhance incident response.
Systemic changes to improve staffing adequacy and support for group homes, including policy reforms and financial investments, are likewise an important step in the right direction. The pandemic has shown that community-based solid care is a must. The importance of collaboration between healthcare providers, policymakers and community stakeholders is to establish robust staffing and care quality standards. Addressing these challenges provides a framework for improving safety and reliability in group home settings, ensuring that residents receive timely and effective care during both routine operations and unexpected events.
The low-hanging fruit in these scenarios are the family caregivers, but they need to have some form of healthcare community outreach education so they can receive information, and perhaps training, that they need to manage the complex care regimens of family members. There is a need to advocate for the roll-out of educational tools for family caregivers who can be instrumental in meeting some of the challenges of chronic wound care in the community.
EDUCATION IS KEY
The article “Teaching Wound Care to Family Caregivers” by Kirkland-Kyhn et al. (2018) highlights the importance of training family caregivers in wound care for patients transitioning from hospital to home. It emphasizes that caregivers often lack adequate preparation, which can lead to complications or poor healing. The authors discuss strategies to improve caregiver education, such as hands-on training, written instructions and follow-up support, to ensure optimal wound care and reduce caregiver stress. The article aims to bridge the gap between healthcare providers and caregivers to enhance patient outcomes.
Discharging patients with conditions requiring ongoing care poses significant challenges, as caregivers may feel unprepared or lack the confidence to manage wound care effectively. This resource emphasizes the importance of comprehensive caregiver education, which includes hands-on training, clear instructions and access to follow-up support.
By utilizing the strategies outlined in this article, case managers can develop individualized discharge plans that empower caregivers, reduce hospital readmissions and improve patient outcomes. The information can be integrated into discharge planning processes to ensure caregivers are well-equipped to handle dressing changes, monitor for signs of infection, and adhere to prescribed care routines. Furthermore, this approach aligns with patient-centered care goals by addressing both the medical and emotional aspects of transitioning home, thereby promoting a safer and more effective recovery process.
Additionally, I co-wrote an article, “Post-Acute Transitional Services: Safety in Home-Based Care Programs” (2022), published on PSNet by the Agency for Healthcare Research and Quality, that explores the critical role of safety in transitional care programs for patients returning home after hospitalization. It emphasizes that while home-based care programs can reduce hospital readmissions and improve patient outcomes, they require careful planning and risk mitigation to address the unique challenges of providing complex medical care in non-clinical environments. The article underscores the importance of structured transitional services, including proper patient assessment, caregiver education and continuity of care.
The authors discuss how successful home-based care programs rely on effective communication between hospital teams, home care providers and family caregivers. By ensuring patients have clear care instructions and caregivers are adequately trained, these programs can enhance safety and quality of care. The article highlights specific safety concerns, such as medication errors, infection risks and inadequate monitoring, that must be addressed to prevent adverse events. It calls for a patientcentered approach that tailors care plans to individual needs while incorporating robust safety protocols.
Ultimately, integrating technology such as telehealth and electronic health records to support seamless communication and improve care coordination is an integral part of this movement. Ongoing research and the development of best practices to optimize home-based care safety are recommended. The development of resources for healthcare professionals, specifically case managers, seeking to design or enhance transitional care programs, ensuring that patients receive safe, high-quality care as they recover at home, is a must.
CASE MANAGERS’ CRUCIAL ROLE
Case managers play a crucial role in the transition of care by ensuring that patients move seamlessly and safely between different levels or locations of care, such as from hospital to home, or from acute care to a rehabilitation or skilled nursing facility. Their responsibilities involve coordinating, planning, and managing all aspects of the patient’s care to promote recovery, prevent readmissions and ensure continuity of services. Below are key roles case managers fulfill during care transitions:
Case managers act as a central point of communication between the patient, healthcare providers, caregivers and community resources. They ensure that all necessary services, such as home health care, physical therapy, wound care or durable medical equipment, are arranged before discharge. This includes facilitating appointments, securing transportation, and ensuring patients understand their medication regimen and follow-up care instructions.
After discharge, case managers monitor the patient’s progress and intervene when necessary to prevent complications or readmissions. This may involve conducting follow-up calls, coordinating home visits by healthcare professionals or ensuring that the patient complies with their care plan. They work to address any new challenges that arise, such as medication issues or worsening symptoms.
One of the most critical roles of a case manager is to minimize risks associated with care transitions, such as medication errors, missed follow-up appointments or lack of proper equipment. By focusing on safety and quality, case managers help reduce hospital readmissions and improve overall patient outcomes.
In summary, case managers act as the patient’s guide and advocate during transitions of care, coordinating services, educating caregivers and ensuring continuity and safety. Their efforts bridge gaps in care, support recovery and enhance the patient’s experience during vulnerable periods.
REFERENCES
Kirkland-Kyhn, H., Generao, S. A., Teleten, O., & Young, H. M. (2018). Teaching wound care to family caregivers. American Journal of Nursing, 118(3), 63—67. https://doi.org/10.1097/01.NAJ.0000530941.11737.1c.
Kirkland-Khyn, H., Teleten, O., Joseph, R., & Maguina, P. (2019). A descriptive study of hospital- and community-acquired pressure ulcers/injuries. Wound Management & Prevention, 65(2), 14-19. https://doi.org/10.1016/j.wmp.2019.02.004.
Kirkland-Kyhn, H., Teleten, O., Joseph, R., & Schank, J. (2019). The origin of present-on-admission pressure ulcers/injuries among patients admitted from the community: Results of a retrospective study. Wound Management & Prevention, 65(7), 24-29. https://doi.org/10.1016/j.wmp.2019.07.006.
Kirkland-Kyhn, H., Howell, M., Senestraro, J., & Walsh, S. (2021). Leveraging technology to improve wound care delivery and care transitions. Nursing Management (Springhouse), 52(11), 24-28. https://doi.org/10.1097/01.NUMA.0000795592.38063.7c.
McElroy, V., Ordona, R. B., & Bakerjian, D. (2022). Postacute transitional services: Safety in home-based care programs. PSNet [Internet]. Rockville, MD: Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services. https://psnet.ahrq.gov/.
Ordona, R. B. (2024). Transition of care challenges and opportunities for chronic wounds. Nursing Clinics of North America. https://doi.org/10.1016/j.cnur.2024.07.014.
Ordona, R., & Bakerjian, D. (2024). Managing care challenges in a group home setting: Is staffing adequate for unplanned incidents? PSNet [Internet]. Rockville, MD: Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services. https://psnet.ahrq.gov/.

, DNP, FNP-BC, GS-C, WCC specializes in delivering communitybased care to vulnerable populations. He co-chairs the GAPNA Home Health and Hospice Coalition and the CANP Health Policy and Practice Committee. In clinical practice, Ordona focuses on transition of care services for patients with chronic wounds and co-morbidities like tracheostomies and ventilator dependence. His nurse-led congregate living health facility was featured in the Sacramento Bee (July 2021). Ordona was awarded the AANP State Award for Excellence in 2022 for his health policy and advocacy work and the GAPNA Excellence Award in Clinical Practice in 2021 for home-based primary care.
Image credit: ISTOCK.COM/BSD555
The post Chronic Wounds: A Case Manager’s Challenge in the Transition from Acute to Community-Based Care appeared first on Case Management Society of America.